



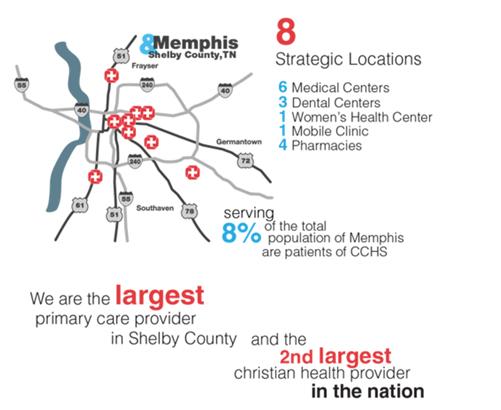
This summer I spent two weeks in Memphis Tennessee. I did a two week rotation with Christ Community Health Services (CCHS). CCHS serves 8% of the population of Memphis, one of the poorest metro cities in the nation. In fact 92% of CCHS’s patients live below the national poverty level. Most of the 162,000 patient visits are with the uninsured or with those on Medicare/Medicaid. Christ Community goes beyond treating the underserved: CCHS believes they have the most impact on their patient populations when they live in the communities of their patients, and are active in their neighborhoods. Consequently, all the staff members of CCHS live in the different communities in which they work (there are 8 different clinics in 5 different neighborhoods). I lived in the neighborhood called Orange Mound. As a student, I rotated in the 8 medical clinics while practicing my medical skills and learning how to counsel patients in mental, emotional, and spiritual health.



Orange Mound
On weekends or in the evenings, students worked in CCHS’s community garden or played with the local neighborhood kids. Everyone in the neighborhood knew about the medical girls on the corner. Neighbors would come by to have their blood pressures taken. Kids would want help with homework or band-aids (and popsicles). Even when we were too busy to play with the children, they would hang out on our front porch because they knew it was a safe place.
As I lived in Orange Mound, my eyes were opened to the struggles of a social class that I was unfamiliar with. Gunshots were fired on our street. The house on the corner was known for its drug dealing and prostitution. My belief that “anyone can make it if they work hard” was challenged. I saw firsthand how individuals are genuinely stuck in their condition: schools get low funding and poor teachers, so valedictorians get ACT’s of 18. Parents have to work several minimum wage jobs to pay rent, and cannot afford to go to school. I saw how the educational and healthcare systems have failed. I also saw nurses, physician assistants, office managers, doctors and their families fighting to better the broken systems. Doctors tutored high school kids and PA students gave up study time to babysit for free while mothers were working. Nurses teamed up with the local school system to push for changing the educational system. I learned how caring for a person’s health means caring for their physical ailments, but also crying with them or cheering them on as they get their GED. I learned that community gardens not only provide food, but also exercise and education. I learned that I don’t have to travel to a different country to find those who are in desperate need of care. My time in Memphis showed me a new way to practice medicine. A way that may result in a smaller house, lower income, and older car, but a way that I believe is richer because of the investment in the relationships with the people around you. I learned that sometimes you must lose to win.
Find out more about Christ Community Health Services at http://www.christcommunityhealth.org/who-we-are/

Anna Quantrille
Anna Quantrille is second-year medical student at the University of South Carolina School of Medicine Greenville.
Copyright 2021 USC School of Medicine Greenville

